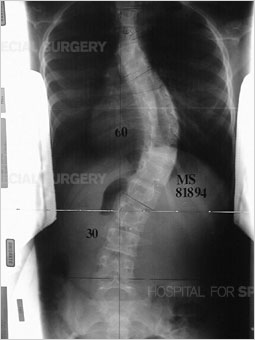
Before I describe what it was like after surgery, here are my x-rays before the operation.
My three curves were measured 34 degrees, 54 degrees, and 28 degrees, from top to bottom. Because that 54 is clearly above the 45-50 degree operative level, that meant I needed surgery. However, because I also had a chiari malformation (when the brain tissue extends into the spinal canal) I needed another surgery. I talked about this in an earlier post, how the brain tissue can cause syrinx (pockets of spinal fluid) to build up in the spine, and that can be dangerous for spinal fusion patients.
In my last post I talked about before the surgery, but now I'll talk about what happens after.
Most people stay in the ICU for one day, although Dr.Shindell is working to find a way to make that not necessary, where they're under high surveillance. Within the first day following the surgery, the doctors have the patient start walking, though with some assistance. I, on the other hand, had to stay in the ICU for two days, as I had a severe drop in blood pressure, causing me to go blue, and causing my parents to have to wait to see me for a few extra hours after.
I wish I could say that I remembered the hospital visit, but I don't, not one bit of it, so here's what my dad said about what I was like,
"You were very antsy, and wanted to be moved around every five minutes, most likely because your body was getting used to being at a different angle. You kept asking to be adjusted. We didn't know if your body was producing cortisol (the hormone they thought was causing your drop in blood pressure). You were very emotional, you wanted to make sure you weren't being a burden. You walked as fast as possible when they asked you to walk because you hated it."
Following about 6 days in the hospital, I was sent home, with a walker, and pain medication (which I didn't take much of after a little while).
For about three weeks, I was in bed, and occasionally following that time, I would leave my bedroom and start walking with the walker, only to sit in the living room chair instead, just for meals.
I didn't eat much, and lost about 11 pounds following the surgery.
Because they thought my body wasn't producing cortisol, they put me on a medication to try and boost the levels of that hormone, and even sent me around with a needle and liquid medication just in case I passed out.
I wasn't allowed to carry anything over 10lbs, and I very often got tired. My muscles ached more than anything, as they cut through a lot of muscle to get down to your spine. Even to this day, over 3 months since the surgery, I still get severe muscle pain in my shoulders when I do too much.
There's so much more that I experienced after the surgery that I either don't remember, or don't want to overwhelm you with, but I feel that these past two blog posts have been pretty informative.
Here is my spine now.
The curve is 28 degrees, which is very good, as very few surgeries actually get full fusion.
The reason I'm trying to study the complications now, is because I had a preoperative condition, and I had postoperative complications (the very low blood pressure) and I wanted to know if they are connected.
I still struggle with data, but with the small amount that I have plus some readings I found, I should be able to get some understanding, but of course this is just a high school project and not an actual government funded research.